Heartless Compassion
It took a lot longer than I anticipated, but my musings about COVID19 and how it affects people and populations in a setting like ours are no longer speculative.
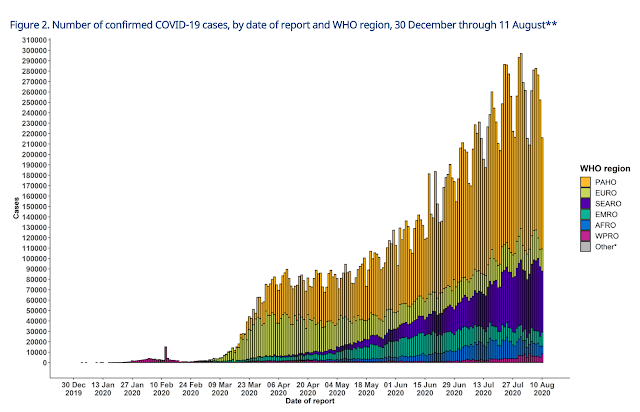
After "appearing" to miss the pandemic, our island nation in the Pacific has caught up lately. After smoldering case numbers, there has been a recent exponential growth in infections, cases and deaths. Because we were so late to the party, multiple vaccines are already available that are both safe and effective at reducing cases and practically eliminating severe disease or death. There's just one problem:
We can't get any.
As case numbers skyrocketed, a more wealthy neighbor brought in a few thousand doses. These were reserved for the capitol city where most of the deaths have been recorded (with an unquantified "batch" set aside for a mining company which threatened to suspend its operations if they didn't get any - simultaneously pointing out how much money they brought into the country). Allegedly, nearly half a million doses will be brought in before year's end through the COVAX scheme. Whoops - the countries which control manufacturing have actually decided to ban exports of those vaccines until they feel like they have their own outbreaks under control. So it looks like this will be another tropical disease that will kill poor folks while more affluent or powerful nations seek to eliminate it as a major public health threat to their people. A sympathetic international organization in the capitol sent us some body-bags, though. Thanks.
So what does it actually look like?
COVID can be pretty nasty. The patients in our isolation ward range from late 30's to early 70's. In our setting they get oxygen, steroids, aspirin, paracetamol (tylenol) and usually an antibiotic that would cover a super-infecting pneumonia. Our nurses and doctors have a "staging area" where they wash up and dress up before going inside. Oxygen levels are checked, concentrators are adjusted, medicine sheets are reviewed, prayers are said. Take all the fixings off - wash up. Back to the wards, ER, delivery beds, operating rooms or clinic. Masks are required for everyone inside the facility (cloth or medical - whatever you can get).
And the work goes on. Car accident victims. Complicated deliveries needing surgeries and blood transfusions. Children dying of diarrhea and malnutrition. TB. HIV. Cancer. Tribal violence. There is a sprinkling of COVID throughout the day. Most mild or moderate cases are seen in the outpatient department who get discharged with paracetamol and 10 days off "work". Others who are severe get admitted into isolation. A few have died so far. Some who would be considered higher-risk have impressed us and survived and gone home. Several staff have been infected and recovered and are back at work.
I am in the line of fire now, as it were. I hope to receive the vaccine as soon as someone with enough authority feels like my safety as a health worker in a poor country is worth the time and energy it would cost to get one to me. How do I feel about the threat and reality of COVID now?
In the past I emphasized the need to preserve essential functions in health systems in the face of COVID. This is still true.
"Paying too much attention to the individual visible victim rather than to the numbers can lead us to spend all our resources on a fraction of the problem, and therefore save many fewer lives. This princple applies anywhere we are prioritizing scarce resources. It is hard for people to talk about resources when it comes to saving lives, or prolonging or improving them. Doing so is often taken for heartlessness. Yet so long as resources are not infinite - and they never are infinite - it is the most compassionate things to do to use your brain and work out how to do the most good with what you have."
-Hans Rosling
Let me illustrate.
A little baby we will call "Susan" came to the hospital today. She was post-ictal from a seizure and had a high fever after a week of coughing at home. She was born 6 months ago in a corner of our province without reliable running water or electricity. Her mother delivered her at the local health center, but the clinic did not have a functioning refrigerator to supply vaccinations. Like most of the infants in that area, she simply went without.
The cause of her cough was a little bacteria called Streptococcus pneumoniae.

In addition to chest infections, it can spread and aggressively attack the body resulting in meningitis.
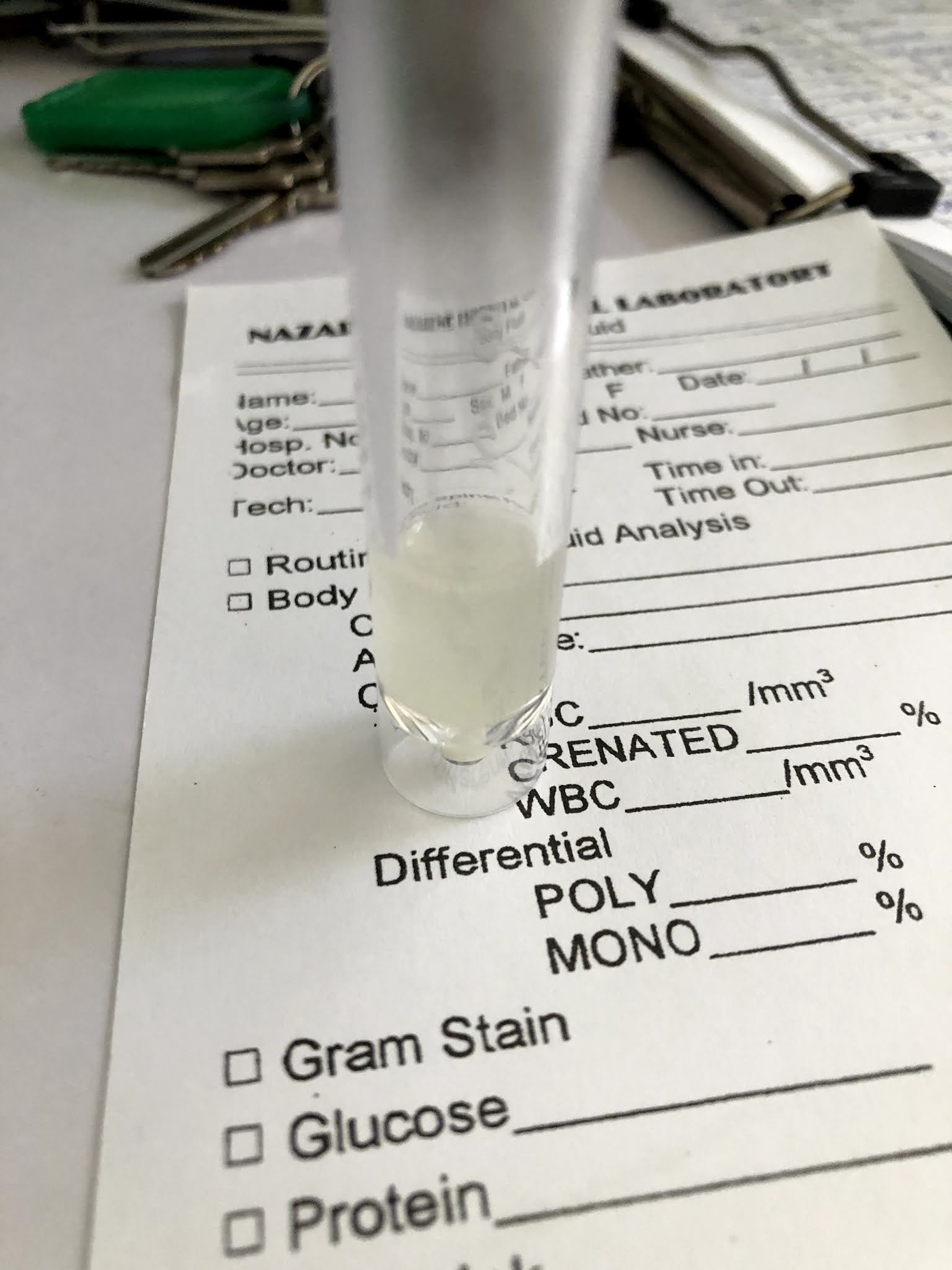 |
| A more macroscopic look at what S. pneumo did to Susan's cerebro-sinal fluid |
Once this happens the infection is severe. The brain is inflammed resulting in seizures and altered consciousness. The treatment is to give powerful antibiotics through intravenous infusion along with steroids, which may help long-term outcomes, and medicines to control seizures.
 |
| Antibiotic, anti-seizure medicine and steroids (does that steroid look familiar?) |
But why didn't I see this in the US? Why was this such a novel thing to learn about when I moved to the tropical jungles of an impoverished nation?
 |
| Before they got all coupled-up with BioNTech |
The vaccination for S. pneumo has been around a while. In fact, this box is from our refrigerator ... located about a 40-minute 4-wheel-drive ride from Susan's health center. But the logistics of getting reliable electricity and a refrigerator there have proven too difficult (or perhaps not "cost-effective" enough) for the various stake-holders to make it happen. I wonder what the company that made this box is busy doing these days ...
Microbes. Body fluids. Medicines. Vaccinations. These are the kinds of things that global health "experts" like to look at and to talk about. What is this germ? Where did it come from? How is it transmitted? What drugs do we have that can help us fight it? When will we get an effective vaccine, for Pete's sake!?
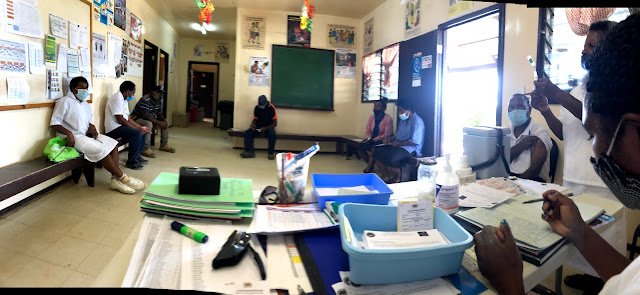
But the people who are on the "front lines" of COVID right now are looking at this:
 | ||
| Susan's mother dutifully wearing a mask to reduce transmission of COVID19 while she watches her daughter dying from a(nother) vaccine preventable disease. |
There is a great line in Harry Potter and the Deathly Hallows that I have consistently thought of lately. Ron, one of Harry's friends, is exasperated that in their desperate struggle to overcome the evil wizard, Voldemort, they are making so little progress and their big "breakthrough" is to learn that there is an object they can use to defeat him ... but they have no idea where it is.
"Don't expect me to be grateful just because there's another damned thing we've got to try to find."
International organizations have set up a template of surveillance that revolves around testing, contact tracing and isolating cases of COVID19. They've even built an app for that. When you transport that into a society where people do not, and cannot, reasonably isolate when they have mild (or no) symptoms you are asking for trouble. You are handing a health system which is already busy chasing TB, HIV, malaria, polio, measles and myriad other infections just another "damned thing to find". Let me save you the suspense: COVID19 is everywhere. There is community transmission in just about every country in the world. It is endemic.
So what is the exit strategy for the new endemic? Thankfully, we already have it! If a vaccine can turn a potentially deadly disease (for maybe 2-5% of the people who are infected with it) into a common cold, it becomes a non-issue. Every dollar that is spent on testing, contact tracing, isolating and repeating the cycle should be immediately funneled into making vaccines, making more of them, making them actually practical in places that may not have a lot of electricity, and making them palatable to the populations you are trying to inoculate.
If and when this is done, all the other things that are killing people at unbelievable rates in the majority world can get the attention and funding they need.
Unfortunately, our global health paradigm is not built for this. Countries with the knowledge and resources to create and manufacture vaccines have made deals with those private companies to supply their own people first, bypassing the vehicle through which the entire world might have had access to a life-saving, and life-normalizing, immunization. The current global health apparatus is built by keeping wealthy people in movie theaters or in stadiums at the Olympics, rather than keeping babies like Susan alive. The challenge of COVID19 has not brought solidarity to a globalized world - it has dropped a greater wedge into the chasm of inequality between the global haves and have-nots. It is easy to overlook this as wealthier countries celebrate their success, take their masks off and go out to restaurants. But overlooking it means we have learned nothing.
There is a chance I will get COVID19. I am being as cautious as I can be. But I cannot "tele-medicine" a C-section or setting a bone. I have a low risk of getting severely ill or dying from it. I am 38, healthy, exercise three times a week, and the usual cold hits me less than the average person. But the risk isn't zero. I could make it practically zero by getting immunized against COVID19 and I plan to do so as soon as it is offered to me. But the reality of health-workers in the 2/3rds world is that we are up against it every single day. The diseases are deadly and we could catch some of them. The outcomes are terrible at times. The systems are inadequate (and sometimes corrupt). On top of that - the more affluent world is pretty much negligent to our realities and probably, for the most part, prefer to keep it that way.
But COVID19 is not the only thing killing our patients and our communities. In fact, it may not be the worst thing affecting them - especially the young families trying to keep the fabric of society alive by working and raising their children to be safe and healthy. The best way out of this mess for these societies has existed for dozens of other diseases for decades - but they march their own paths of destruction through lives, families, communities and countries at alarming rates compared to the OECD nations. While SARS-COV-2 is a "novel" pathogen, the reality it generates is not that "novel" for those who watch their children die of other preventable diseases. Tragically, they have grown accustomed to living (or dying) with the daily miseries that come from inadequate treatment, out-of-reach vaccinations and a global neglect that changes slowly - if at all. The old paradigms of "Global Health" or "Tropical Medicine" or "International Health" are not serving them very well at the moment.
If COVID19 cannot be a bridge, perhaps it can be an alarm bell.

Comments
Post a Comment